Addressing Critical Unmet Needs in Musculoskeletal Medicine
Medical practice planting and administration. My initial experience involved establishing a solo practice, followed by development of a specialty building across from the hospital Emergency Department. In Bloomington, Indiana, during a period of personal loss, I found key opportunities and mentoring in care delivery. By accepting each opportunity and applying broad training, I became the region’s busiest surgeon. I inherited proactive staff who contributed practical methods. A second practice planting after more than a decade in academia, alongside colleagues leaving the University, addressed emerging economic challenges. As volunteer vice chair of orthopedics at a community hospital, surgeon recruitment for call coverage proved difficult amid population growth, underprivileged patients, declining reimbursements, and redirected federal funding. Hospital instability continued with loss of OR access and referral shifts to hospital-based systems. Flexibility and availability to hospitals requiring broad surgical coverage have sustained my clinical practice into later career stages.
Bench research. Beginning in medical school and continuing through fellowship and postdoctoral orthopedic research, I conducted cell and animal studies, including grant management as U.S. funding declined. I collaborated with industry in product development and testing, including electrical tissue stimulation and first clinical wound use of recombinant peptide BMP-2.
Clinical research. Using early computerized clinical data, I documented long-term outcomes of shoulder injury in geriatric surgical patients. This work supported roles as orthopedic EHR liaison, quality officer, and leader of outcome and efficiency studies across multiple EHR platforms.
Mechanical analysis, implant design, and testing. My early faculty work addressed calcaneus central depression fractures and unstable intertroch/subtroch hip fractures. These were modeled, implants developed and tested, resulting in a patented calcaneus implant and hip implant advancements widely used today.
Wound biology and local modulation of healing. At UPenn, guided by leaders in orthopedic research, I earned an advanced degree based on original work on microvessel ingrowth in bone formation. Postdoctoral work expanded this to growth regulation, recombinant therapies, and extracellular matrix biology. Facing severe wounds with high infection rates, I led development of resorbable polysaccharide wound implants for environmental restoration and antibiotic delivery. These showed high efficacy in animal studies and, under IRB oversight, in clinical trials.
Current projects at OrthoAgile:
- Anatomic Rotator Cuff Arthroplasty (ARCA): A patented anatomic shoulder replacement capable in rotator cuff deficiency, enabled by Patient Match technology and enhanced glenoid fixation. Prototypes confirm surgical feasibility. Regulatory guidance supports a 510(k) pathway, initially marketing a specialty baseplate for Reverse Shoulder Replacement with future expansion to full anatomic replacement.
- Wound gel: A locally applied wound-care product encouraged by the U.S. Department of Defense for battlefield use. Open fractures remain disabling and costly for veterans.
- Osteotomy device: A computer-guided, infinitely adjustable system enabling durable correction with early return to function.
- Robot-guided knee replacement: An approach designed to reduce surgical trauma, infection, and arthrofibrosis, major contributors to unsatisfactory outcomes.
Innovations and Patents
A Bone Buttress Plate for Calcaneus - Patent No. - 6123709
Often considered a debilitating injury due to heel shortening, complex calcaneal fractures lack a consistently effective surgical solution. We are developing a breakthrough operative approach grounded in detailed biomechanical force analysis. This evidence-based methodology allows for restoration of calcaneal height and alignment, fundamentally improving patient outcomes, through the use of our patented plate-and-screw tabletop construct.
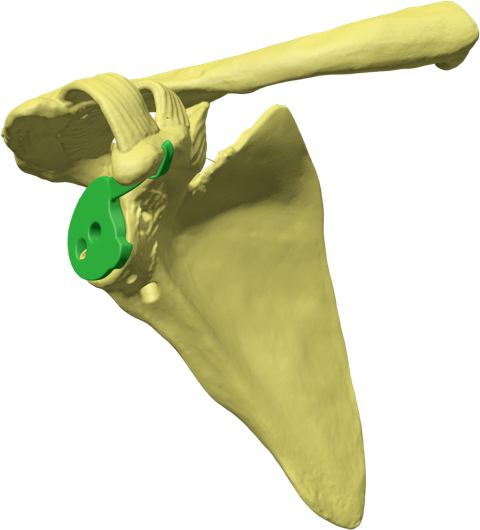
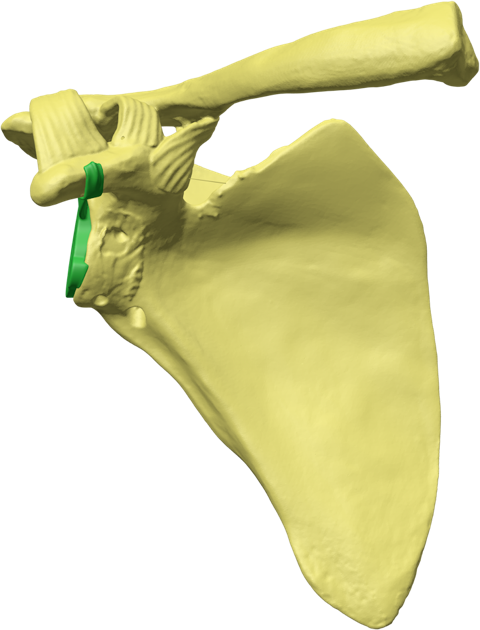
Glenoid Fixation Challenge - Patent No. - US11918476B1
In shoulder arthroplasty, achieving durable glenoid implant fixation remains a key unmet need. Although current techniques continue to advance, they present meaningful limitations—particularly for older patients. Our solution is focused on addressing these challenges through a novel, less invasive fixation approach designed to better support bone ingrowth and long-term stability. With this strategy, we aim to help drive the next generation of shoulder replacement solutions.
Hydrogel Care for Wound Healing
Our team of trauma orthopedists at WakeMed in Raleigh, North Carolina, has investigated polysaccharide gels (Sorbsan) as a wound protectant and localized antibiotic delivery platform. In a hamster model of open femur fractures stabilized with intramedullary fixation, we observed a significant reduction in wound infection rates and verified effectiveness through an IRB-approved clinical study involving trauma patients. Based on these results, the U.S. Department of Defense has invited us to submit an application to adapt this product for field use, with the goal of improving outcomes after severe open-fracture injuries—an area where recovery can be limited and return-to-duty rates remain low.
Narrative and Curriculum Vitae
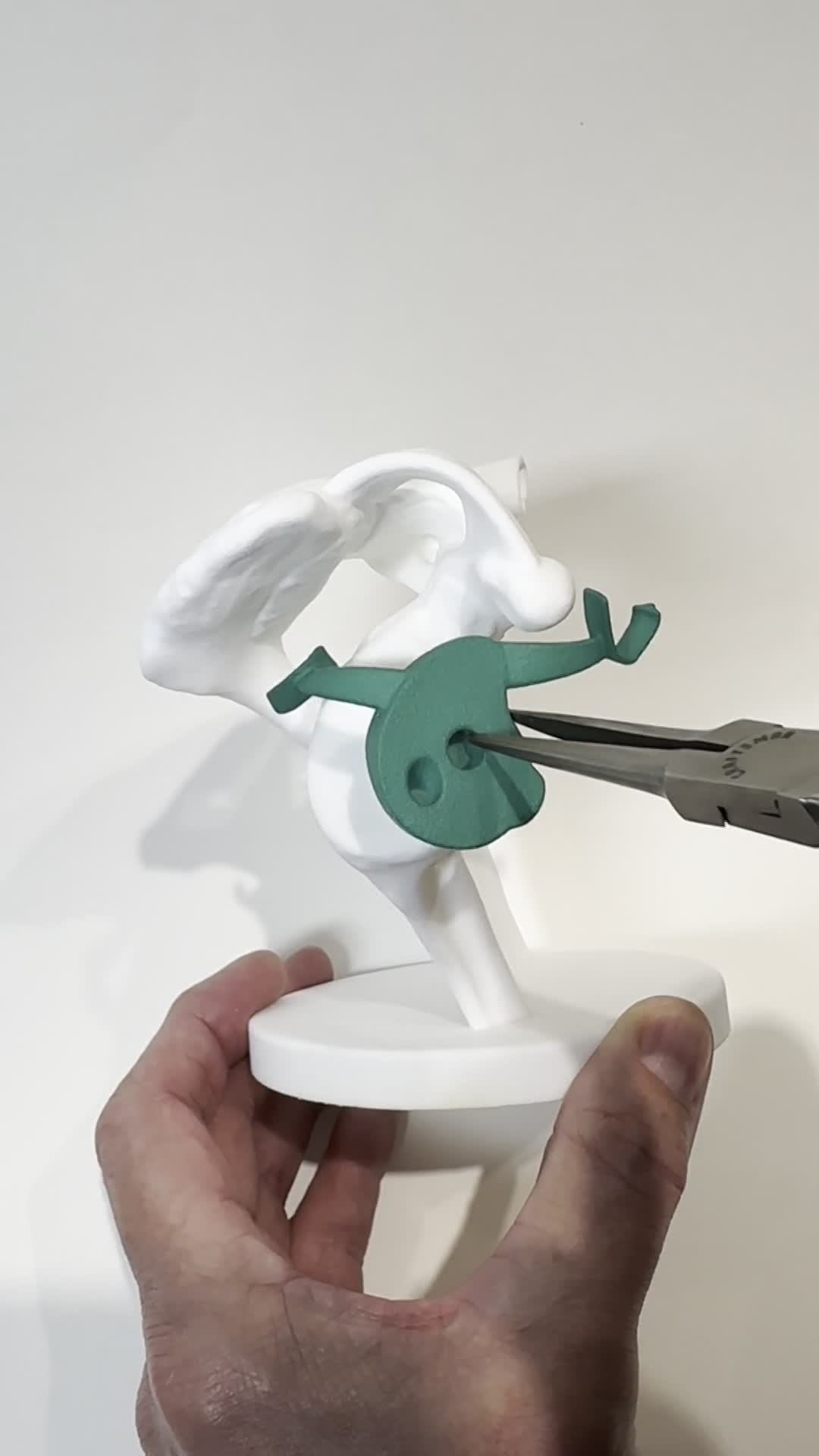
Glenoid Base Insertion
Shoulder Detail Images

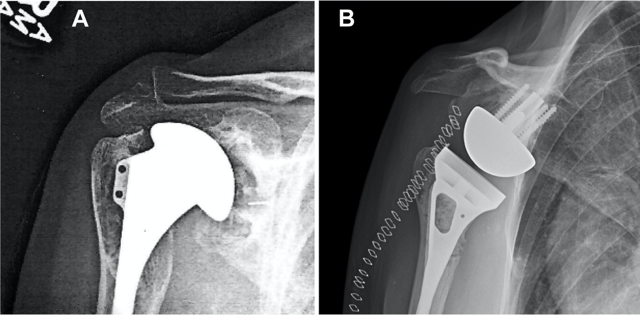
Historical perspective: The injuries shown (see "Gallery" Button - located below text) demonstrate severe fragmentation of the proximal humerus. Prior to the availability of CT imaging to clearly delineate fracture fragments, interpretation relied heavily on surgeon experience to reassemble and stabilize fragments using tools and implants adapted from other anatomic sites.
Today: Modern CT and MRI imaging, along with improved fixation devices such as locked nails and locking plates, have enabled more successful surgical treatments by reducing trauma and improving fracture stability. However, osteoporosis, rehabilitation forces, and delayed bone healing challenge fixation, and failure may occur during early arm use or after a fall. Individualized treatments are often necessary but cumbersome, and insurance considerations may influence operative decisions, as these injuries frequently compromise independent living.
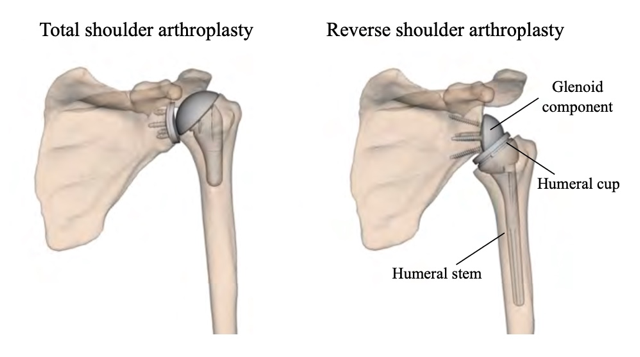
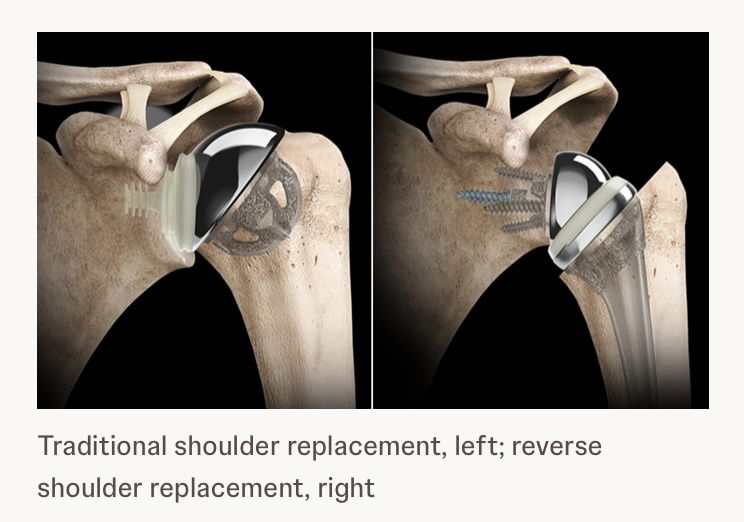
Reverse Total Shoulder Replacement is increasingly used for complex fracture patterns because it can restore painless arm use more reliably in patients with rotator cuff insufficiency. Limitations include reduced overhead motion and risk of dislocation.
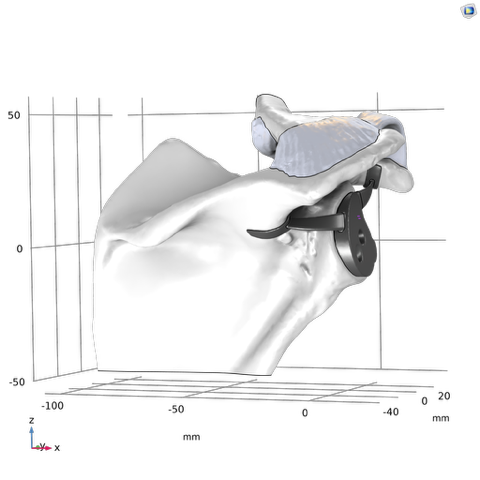
Our innovative design restores anatomic mechanics through enhanced glenoid implant fixation. Using patented Patient Match technology, CT data generate implants matched to variable scapular anatomy, providing immediate fixation that counteracts early rehabilitation forces and supports bone ingrowth into a porous surface for permanent fixation. Improved fixation enables mechanical constraint, supports anatomic shoulder replacement designs, improves motion, and reduces dislocation risk.
The proposed solution, Anatomical Rotator Cuff Arthroplasty (ARCA), reflects unprecendented potential to restore normal shoulder biomechanics for patients requiring joint replacement.